
By Dian Rahmadin Akbar
Definition
Bradycardia is defined as a heart rate less than 60 times a minute. This may be very normal for young people and healthy adults. Normal people generally have a heart rate between 60-100 times per minute. However, in people whose hearts are trained, such as athletes, their heart rate can be less than 60 times a minute. In some cases the heart rate is below 60 beats per minute, for example during deep sleep. In addition, the elderly are more susceptible to problems with a slow heart rate. Although the limit of bradycardia is 60 times per minute, but generally signs and symptoms can arise if the heart rate is less than 50 times per minute (AHA, 2014).
Bradycardia is considered pathological if the cardiac output decreases to the point that will cause symptoms. Pathological bradycardia is most common in older people based on cardiac conduction disorders. It is important to remember that the heart rate is determined by the pulse and not what is displayed on the monitor. For example, a person with a heart rate displayed on an 80 monitor. But if ectopic ventricular contractions are not strong enough to have an effect on blood flow, then the true pulse is 40.
Etiology
There are 2 main etiologies in the occurrence of bradyarrhythmias, namely disorders of impulse formation and impulse conduction disorders.
Impulse Formation Disorders
Sinus Bradikardi
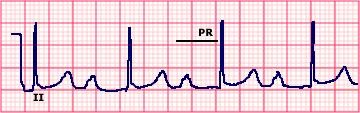
Is a sinus rhythm with impulses <60x / minute. Each P wave is always followed by a QRS gel. PR normal interval. Causes: Hypothermia, vagal maneuver / carotid stimulation massage, parasympathomimetic drugs, hypothyroidism, hypoxemia, IMA, severe shock
Characteristics:
Frequency: slow (less than 60 x / minute)
Rhythm: Regular
P wave: normal
PR interval: normal (0.12-0.20 seconds)
QRS: normal (0.06-0.10)
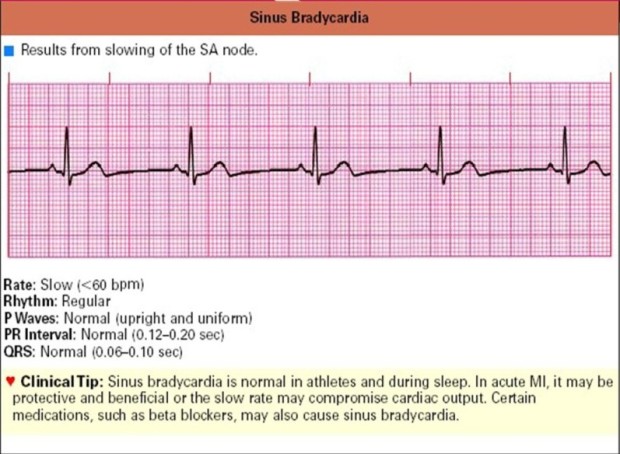
Sinus bradycardia is normal in athletes and during sleep. It is also possible to occur in acute myocardial infarction. Certain medications, such as beta blockers, can also cause sinus bradycardia
Sick Sinus Syndrome
Sick sinus syndrome is a set of symptoms caused by abnormalities of the SA node, which include: (1) spontaneous sinus bradycardia, which is not caused by drugs and is not in accordance with physiological conditions; (2) Sinus arrest or exit block; (3) combination of SA and AV conduction disorders; (4) bradycardia-tachycardia syndrome.
Characteristics:
Frequency; atrial 60 x per minute, ventricular 70 x per minute
Rhythm: irregular
P wave: configurations vary
PR interval: with varying rhythms
QRS: normal (0.06-0.10 seconds)
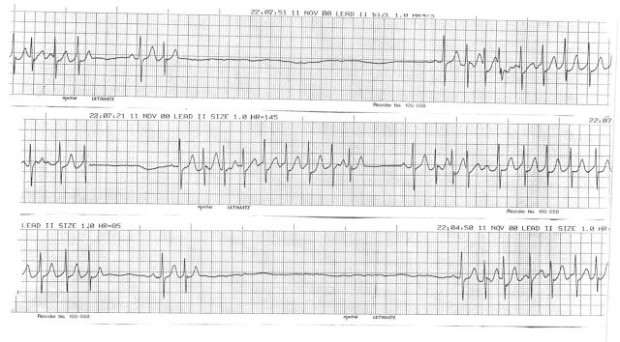
tachydardia-Bradycardia syndrome, namely the presence of a fast heart rate followed by bradycardia to sinus arrest. Caused by malfunction of the SA Node, resulting in an abnormal heart rhythm
Hypersensitive Carotid Sinus Syndrome
Afferent branch hypersensitivity or efferism of the carotid sinus arch reflex causes vagal activation and / or sympathetic inhibition, leading to bradycardia and vasodilation.
Impulse Delivery Disorders
Atrioventricular Conduction Block
AV Block is defined as an obstacle or disruption in the propagation of impulses from the atrium to the ventricles caused by anatomic disorders or functional disorders of the conduction system. This conduction disorder can be temporary or permanent; conduction can only be slowed, only occasionally, or stunted. Conduction disorders are classified into 3 based on severity, namely degrees 1, 2, and 3.
AV Block 1 degree
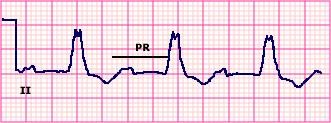
In grade 1 AV block, each impulse from the atrium conducts to the ventricles, producing a sinus rhythm, but with a PR interval> 0.2 seconds. Conduction disorders usually originate from the AV node, and can be caused by transient disorders or due to structural defects. Reversible causes include increased vagal tone, transient ischemic AV nodes, and drugs that can interfere with impulses in the AV node. Structural causes of myocardial infarction, and degenerative diseases of the conduction system, are often seen in older people.
Characteristics:
Rate: depends on the underlying rhythm
Cadence: regular
P wave: normal
P-R interval: lengthwise (> 0.20 seconds)
QRS: normal (0.06-0.10 seconds)
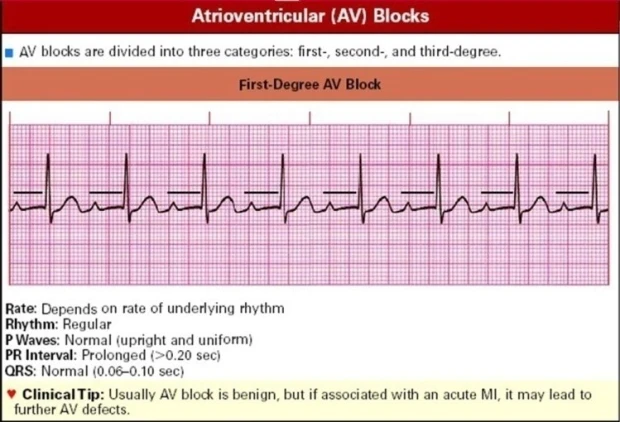
usually AV block is harmless, but if associated with acute myocardial infarction, it can cause further AV damage
1st degree AV block is divided into 3
First Degree AV Block with Sinus Rythm
First Degree AV Block with Left Bundle Branch Block
First Degree AV Block with Infranodal Conduction Delay

AV Block 2nd degree
In grade 2 block, some atrial impulses fail to reach the ventricles. Wenkebach describes a progressive slowdown between atrial and ventricular contractions, and finally the failure of atrial impulses to reach the ventricles using polygraph. Mobitz divides the 2nd degree AV block based on the image on the ECG to 2; that is :
Type I 2nd degree block
Is a phenomenon described by Wenkebach, but in the picture of the ECG; that is, there is a progressive increase in the PR interval followed by P without conduction. Type I blocks generally occur in the AV node, where fatigue occurs with each impulse, which is seen by prolonging the PR interval, and finally blocks occur so that the ECG image shows a P wave without QRS being followed. After this resting phase, the cycle repeats again with the PR interval as before.
Type I 2nd degree block
Characteristics:
Rate: depends on the underlying rhythm
Rhythm: irregular
P wave: normal
P-R interval: increasingly extends until wave P is not followed by QRS
QRS: normal (0.06-0.10 seconds)
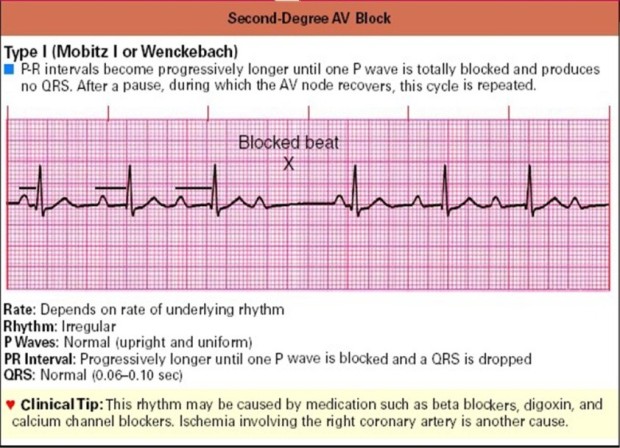
The PR interval extends until the P wave is completely blocked and does not cause a QRS wave. After a pause, this cycle is repeated again. This rhythm may be caused by drugs such as beta blockers, digoxin, and calcium channel blockers. Another cause is ischemia in the right coronary artery
Type II grade 2 block
Block type II has a sudden loss of AV conduction, without the extension of the PR interval. Type II blocks generally originate from conduction blocks on the path below the AV node (Bundle of His, or more distal to the purkinje system). Block type II is permanent and usually develops to a high degree, even to a total block. The first management is to seek and correct reversible trigger factors, such as myocardial ischemia, increased vagal tone, and drug use. If no reversible cause is found, it is recommended not to use drugs that can interfere with AV node conduction and the installation of a permanent pacemaker.
Characteristics:
Rate: more atrial rate (always 60-100), faster than the ventricular rate
Rhythm: regular atrial and irregular ventricular
P wave: normal, more P waves than QRS
P-R interval: normal or elongated but constant
QRS: always widens (> 0.10 seconds)
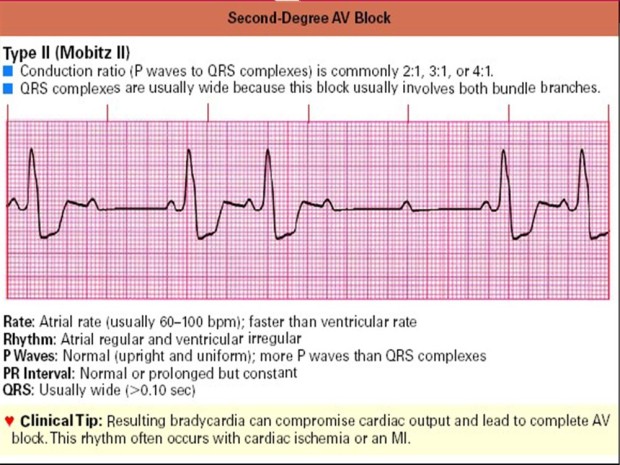
Conduction ratio (P waves followed by complex QRS) are generally 2: 1, 3: 1 or 4: 1. QRS complexes are usually dilated because they involve blocks in both branches of the bundle. This rhythm often occurs in cardiac ischemia or myocardial infarction
3rd degree AV block (Total AV block)
In grade 3 block, there is no atrial impulse reaching the ventricle (P wave is not followed by QRS). In grade 3 block, atrial electricity is not associated with ventricles, where the atrium is depolarized as a response to the SA node, and the ventricles contract based on escape rhythm below the block. This results in ECG images showing P waves with frequencies that are not related to the interval of the appearance of QRS waves. Depending on where the escape rhythm arises, QRS waves can be narrow with a frequency of 40 – 60x / minute (AV rhythm) or if more downward from the system can be slower (His or Purkinje). As a result of contraction out of sync, a decrease in cardiac output can occur; patients can experience dizziness, presinkop, or even syncope. 3rd degree blocks can also result in VT or VF. Management of grade 3 block as in grade 2 block, which starts with correcting reversible causes, and if the pacemaker does not improve can be installed. In the total AV block, a dual chamber pace maker is usually done.
Characteristics:
Rate: atrial 60-100 ventricular 40-60
Rhythm: regular but atrial and ventricular running independently
P wave: normal
P-R interval: normal, may blend with complex QRS / T waves
QRS: always widens (> 0.10 seconds)
There is no conduction between the atria and ventricles because of the electric block. AV block degree 3 is commonly referred to as “complete heart block”.
Conclusion:
Of the many etiologies that cause bradycardia, there is the most dangerous etiology. Two different rhythms are AV degree II and AV block III (total AV block). Both of these rhythms are usually associated with myocardial infarction in the antero septal section
Management
The Bradycardia algorithm in the ACLS outlines steps to assess and manage patients who present with symptomatic bradycardia or bradycardia which causes symptoms of shortness of breath, chest pain, dizziness, decreased consciousness, weakness, or fainting. On examination can be found conditions of hypotension, shock, pulmonary edema and cold akral with decreased urine production. Starting with the decision that the patient’s heart rate is <60 bpm and is symptomatic (AHA, 2015).
The steps to assess and manage include:
- The decision that the heart rate is <60 bpm and is symptomatic.
- Assess and manage patients using primary and secondary surveys:
- Maintain a patent airway.
- Helps breathing when needed.
- Give oxygen if oxygen saturation is less than 94% or the patient is short of breath
- Monitor blood pressure and heart rate.
- Install 12-lead ECGs
- Installing access IV.
- History of problem focus and physical examination.
- Search for and deal with factors that might contribute.
- Answer two questions to help you decide whether the signs and symptoms of poor perfusion are caused by bradycardia.
- Are there serious signs or symptoms, such as hypotension, pulmonary congestion, dizziness, shock, ongoing chest pain, shortness of breath, congestive heart failure, weakness or fatigue, or changes in acute mental status?
- Are the signs and symptoms associated with a slow heart rate?
- Are there other reasons for the patient’s symptoms to arise other than due to a slow heartbeat.
- Determine whether the patient has adequate or less perfusion, because the order of treatment is determined by the patient’s clinical severity.
- If perfusion is adequate, monitor and observe the patient.
- If perfusion is poor, move quickly through the following actions:
- Preparing transcutaneous pacing. Don’t delay pacing. If there is no transcutaneous pacing IV being the first choice.
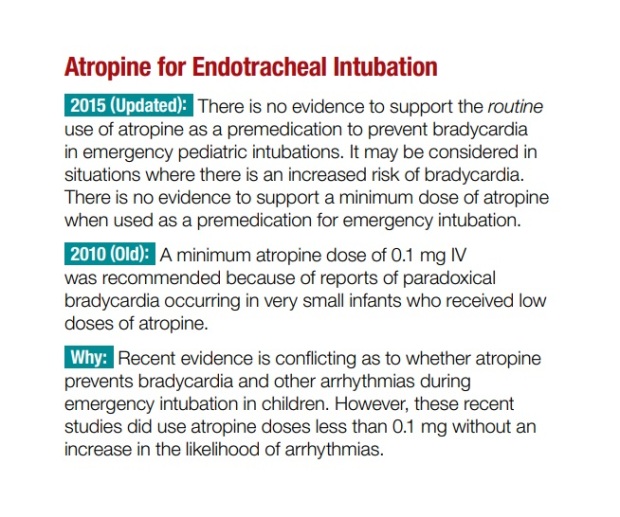
- Consider giving atropine 0.5 mg IV if IV access is available. Repeat every 3 to 5 minutes for 3 mg or 6 doses.
- If atropine is not effective, start pacing.
- Consider epinephrine or dopamine while waiting for pacing or if pacing is ineffective.
- Epinephrine 2 to 10 µg / minute
- Dopamine 2 to 10 µg / kg per minute

Therapy
Giving therapy according to the etiology found
In dealing with patients with bradycardia the important thing is to determine whether bradycardia has caused symptoms of heart rate <60 times per minute, shortness of breath, chest pain, dizziness, decreased consciousness, weakness, almost fainting until fainting. If so, try to increase your heart rate with the following steps:
– Immediately make sure there are no airway disorders
– Give oxygen
– Install an ECG monitor, blood pressure and oximetry
– Install the IV line
Pay attention to ECG:
If the EKG is not AV block II type 2 or total AV / degree 3 do the following steps:
- Give sulfas Atropine 0.5 mg IV while observing the ECG monitor to see a response to an increase in heart rate, if there is no repeat 0.5 mg (every 3-5 minutes), until there is an increased response to heart rate or the dose of atropine has reached 3 mg.
- If the atropine suldaf dose has reached 3 mg and there has not been an increase in heart rate> 60x / minute, consider giving other drugs such as epinephrine 2-10 microgram / minute or dopamine 2-10 microgram / kgBB / minute.
If the EKG picture is block type II type 2 or total AV / degree 3 do the following steps:
- Immediately install a transcutaneous pacemaker while waiting for the installation of a tranvesa pacemaker (Consult a cardiologist)
- Look for and treat causes that can support such as hypoglycemia, hypokalemia, hypovolaemia, acidosis, cardiac tamponade, trauma.
Stages of treatment options for bradycardia
1. Atropin
In the absence of reversible causes, atropine remains the first-line drug for acute symptomatic bradycardia (Class IIa). Atropine is useful for treating symptomatic sinus bradycardia and may be beneficial for any type of AV block. Atropine dosage is recommended for bradycardia 0.5 mg IV every 3 to 5 minutes for a maximum total dose of 3 mg. The dose of atropine sulfate ≤ 0.5 mg may be paradoxical which results in a slowdown in administration of atropine.
Use atropine carefully in acute coronary ischemia or myocardial infarction. An increase in heart rate may worsen ischemia or increase the infarction zone. Avoid relying on atropine for AV degree II and III blocks. Patients like this need immediate pacing.
2. Transcutaneus Pacing
Immediately start transcutaneous pacing in patients who do not respond to atropine. Transcutaneous pacing is a class I intervention for symptomatic bradycardia. This should be started immediately for unstable patients, especially in high-AV blocks (AV Block Mobitz II degree II or third). If the transcutaneous worm is ineffective (for example, inconsistent capture), then it is prepared for transvenous pacing and consult an expert. For patients with symptomatic bradycardia with signs of low perfusion, transcutaneous pacing is the treatment of choice.
3. Epinefrin
Infusion epinephrine can be used for patients with symptoms of bradycardia or hypotension after failed atropine or pacing (Class IIb). Start infusion at 2 to 10µ gr / minute. Dosage titration to assess patient response, intravascular volume and support needed.
4. Dopamin
Dopamine hydrochloride has good action on α and β adrenergic. Dopamine infusion (at levels of 2 to 10 micrograms / kg per minute) can be added to epinephrine or given alone. Dosage titration to assess patient response, intravascular volume and support needed (AHA 2005).
Primary Survey
- Airway: assessment of patency of the airway, including examination of the presence of airway abortion, due to foreign objects. For clients who can speak, it can be considered that the airway is clean. Also conducted is the assessment of the presence of additional breath sounds such as stridor.
- Breathing: inspection of breath frequency, whether there is use of respiratory aids muscles, shortness of breath, palpation of pulmonary development, auscultation with additional breath sounds, such as ronchi, whezzing, assess for chest trauma that can cause tachypnea and dispneac.
- Circulation: an assessment of blood volume and cardiac output is carried out as well as bleeding. Hemodynamic settings, skin color, blood pressure, pulse (assessing shock signs).
- Disability: the value of the level of consciousness and the size and reaction of the pupil.
Secondary Survey
- History: related to complaints and symptoms, past medical history and related family and causes aterioventricular 1st degree block arrhythmias, Anamnesis can use AMPLE format (allergies, Medication, Post Illnes, Last meal, and Event / Environment related to the event).
- General physical examination starts from the head to the feet, a physical examination of the torax is:
- Inspection: are there any abnormalities in the shape of the chest wall
- Palpate: to feel if there is crepitation on the Os. Costa, assessing the pressure of the jugular vein, assessing the apex cordis.
- Percussion: assess the heart’s limit, is there an enlargement or not
- Auscultation: assess heart sounds, whether there is an additional sound or not and assess sounds at each valve (aortic valve, pulmonary valve, mitral valve, tricuspid latup) and can also add more diagnostic tests such as ECGs with results that will show whether there is heart blockade or other heart disease, and also can be done thoracic examination to find out if there are abnormalities in the anatomical structure of the heart (such as the size of the heart) or there are other symptoms of damage to other organs.
Supporting investigation
- ECG: shows the pattern of ischemic injury and impaired conduction. Declare the type / source of dysrhythmias and the effects of electrolyte imbalances and heart medications.
- Holter Monitor: An ECG image (24 hours) is needed to monitor the electrical activity of the heart. It can also be used to evaluate pacemaker function / the effects of antidysrhythmic drugs.
- Drug checks: Can state cardiac drug toxicity, the presence of beta blockers, digoxin, and calcium channel blockers that are the cause of bradycardia.
Nursing diagnoses
Decreased cardiac output b / d physiological response of the heart muscle, increased frequency, dilation, hypertrophy or increased stroke
NOC:
- Cardiac Pump Effectiveness
- Circulation Status
- Vital Sign Status
Result Criteria:
|
Indicator
|
Normal condition
|
| Systolic pressure, diastolic |
<110-140 (systolic) / 85 (diastolic) mmHg |
| MAP |
> 60 |
| The frequency of carotid pulses right and left |
60-100 times / minute |
| PaO2 and PaCO2 |
PO2: 80-100 mmHg and PCO2: 35-45 mmHg |
| GCS |
4-5-6 |
| Orthostatic hypotension |
There is no orthostatic hypotension |
| Additional breath sounds |
No additional sound |
| Neck vein distension |
There is no distention |
| Peripheral edema |
There is no peripheral edema |
| CRT |
<2 seconds |
| Akral |
Warm |
NIC:
Cardiac Care
- Evaluation of chest pain (intensity, location, duration)
- Note the presence of cardiac dysrhythmias
- Note any signs and symptoms of decreased cardiac putput
- Cardiovascular status monitoring
- Respiratory status monitor which indicates heart failure
- The abdominal monitor as an indicator of decreased perfusion
- Monitor fluid balance
- Monitor for changes in blood pressure
- Monitor patient response to the effects of antiarrhythmic treatment
- Set the period of exercise and rest to avoid fatigue
- Monitor patient activity tolerance
- Monitor for dyspneu, fatigue, tekipneu and orthopneu
- Advise to reduce stress
Vital Sign Monitoring
- Monitor TD, pulse, temperature, and RR
- Note blood pressure fluctuations
- VS monitor when the patient is lying down, sitting or standing
- Auscultate TD in both arms and compare
- Monitor TD, pulse, RR, before, during, and after activity
- Monitor the quality of the pulse
- Monitor for pulsus paradoxus
- Monitor for pulsus alterans
- Monitor the amount and rhythm of the heart
- Monitor heart sounds
- Monitor the frequency and rhythm of breathing
- Monitor lung sounds
- Monitor abnormal breathing patterns
- Monitor skin temperature, color and moisture
- Monitor peripheral cyanosis
- Monitor for cushing triad (widening pulse pressure, bradycardia, increased systolic)
- Identify the causes of vital sign changes
Intolerance of activity b / d low cardiac output, inability to fulfill skeletal muscle metabolism, pulmonary congestion that causes hypoxinia, dyspneu and poor nutritional status during illness
Definition: Insufficient physiological and psychological energy to continue or complete the requested activity or daily activities.
Limitation of characteristics:
- verbally report fatigue or weakness.
- Abnormal response of blood pressure or pulse to activity
- ECG changes that show arrhythmia or ischemia
- There is dyspneu or discomfort while on the move.
Related factor factors:
- immobilization
- Overall weakness
- Imbalance between suplei oxygen and need
- A lifestyle that is maintained.
NOC:
- Tolerance Activity
- Fatigue Level
Result Criteria:
|
Indicator
|
Normal conditions
|
| O2 saturation in the normal range |
95-100% |
| Pulse in the normal range |
60-100x / min |
| RR when the activity is within the normal range |
12-20x / min |
| Systolic pressure, diastolic in the normal range |
<110-140 (systolic) / 85 (diastolic) mmHg |
| ECG results within normal limits Normal |
rhythm |
|
Indicator
|
Normal condition
|
| Fatigue |
No fatigue |
| Lethargy |
No lethargy |
| decreased appetite Good |
appetite |
| headache |
Scale of pain 0 |
| sleep and rest within normal limits |
5-7 hours / 24 hours |
NIC:
Energy Management
- Observe the limitation of clients in carrying out activities
- Encourage the anal to express feelings towards limitations
- Assess for factors that cause fatigue
- Monitor nutrition and strong energy sources
- Monitor the patient for excessive physical and emotional fatigue
- Monitor cardivascular response to activity
- Monitor sleep patterns and length of sleep / patient rest
Activity Therapy
- Collaborate with Medical Rehabilitation Workers in planning the right therapy program.
- Help clients to identify activities that can be done
- Help to choose consistent activities that match physical, psychological and social abilities
- Help to identify and get the resources needed for the desired activity
- Help to get activity aid tools such as wheelchairs, crutches
- Help to identify the activities you like
- Help clients to make training schedules in their spare time
- Help patients / families to identify deficiencies in activities
- Provide positive reinforcement for those who are active in activities
- Help patients to develop self motivation and reinforcement
- Monitor physical, emotional, social and spiritual responses
References
American Heart Association. 2005. Part 7.3: Management of Symptomatic Bradycardia and Tachycardia. http://www.circulationaha.org. DOI:10.1161/CIRCULATIONAHA.105.166558. Downloaded from http://ahajournals.org by on April 3, 2019. Circulation. 2005;112:IV-67-IV-77.
American Heart Association. 2015. HIGHLIGHTS of the 2015 American Heart Association
Guidelines Update for CPR and ECC. AHA Guidelines Highlights Project Team. 7272 Greenville Avenue, Dallas, Texas 75231-4596, USA. http://www.heart.org
Kusumoto FM et al., 2018, 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay. 2018 Bradycardia Clinical Practice Guidelines. Downloaded from http://ahajournals.org by on April 3, 2019. https://www.ahajournals.org/doi/suppl/10.1161/CIR.0000000000000628.
Shen W-K et al., 2017. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope. ACC/AHA/HRS GUIDELINE. Downloaded from http://ahajournals.org by on April 3, 2019. Circulation. 2017;136:e60–e122. DOI: 10.1161/CIR.0000000000000499











 Sebanyak 123 mahasiswa diangkat sumpah nya kemarin (14/1) di Gedung Gradika Bhakti Praja, Kota Pasuruan. Angkat sumpah dan pelantikan itu disak sikan langsung oleh orang tua ma hasiswa, serta undangan VVIP yang meliputi Plt. Wali Kota Pasuruan diwakili oleh Sekda Kota Pasuruan Bahrul Ulum, Forpimda Kota Pasuruan, jajaran civitas akademika Universitas Jember, Ketua DPW PPNI Jatim, Ketua PPNI Kota Pasuruan, DPRD Kota Pasuruan,
Sebanyak 123 mahasiswa diangkat sumpah nya kemarin (14/1) di Gedung Gradika Bhakti Praja, Kota Pasuruan. Angkat sumpah dan pelantikan itu disak sikan langsung oleh orang tua ma hasiswa, serta undangan VVIP yang meliputi Plt. Wali Kota Pasuruan diwakili oleh Sekda Kota Pasuruan Bahrul Ulum, Forpimda Kota Pasuruan, jajaran civitas akademika Universitas Jember, Ketua DPW PPNI Jatim, Ketua PPNI Kota Pasuruan, DPRD Kota Pasuruan, Yang mewakili Ketua Dewan Pengurus Wilayah PPNI Provinsi Jawa Timur Dr. Ahsan, S.Kp., M.Kes. dalam sambutannya banyak berpesan kepada para petugas kesehatan yang diambil sumpahnya. “Ke depan, tantangan kalian adalah era ketidakpastian. Setiap orang pasti punya pengalaman masa lalu, masa kini, dan menyambut masa depan. Namun, saya bangga kepada kalian semua karena IPK-nya rata-rata sudah di atas 3,5,” ujarnya. Namun, tak hanya cukup bermodal itu. “Ke depan kalian harus memiliki standar serta menjadi pribadi
Yang mewakili Ketua Dewan Pengurus Wilayah PPNI Provinsi Jawa Timur Dr. Ahsan, S.Kp., M.Kes. dalam sambutannya banyak berpesan kepada para petugas kesehatan yang diambil sumpahnya. “Ke depan, tantangan kalian adalah era ketidakpastian. Setiap orang pasti punya pengalaman masa lalu, masa kini, dan menyambut masa depan. Namun, saya bangga kepada kalian semua karena IPK-nya rata-rata sudah di atas 3,5,” ujarnya. Namun, tak hanya cukup bermodal itu. “Ke depan kalian harus memiliki standar serta menjadi pribadi Sekda Kota Pasuruan Bahrul Ulum yang mewakili Plt. Wali Kota Pasuruan Raharto Teno Prasetyo, S.T. mengucapkan selamat kepada seluruh lulusan juga kepada orang
Sekda Kota Pasuruan Bahrul Ulum yang mewakili Plt. Wali Kota Pasuruan Raharto Teno Prasetyo, S.T. mengucapkan selamat kepada seluruh lulusan juga kepada orang Sementara itu, Rektor Universitas Jember Drs. Moh. Hasan, M.Sc., Ph.D. dalam sambutannya menyampaikan apresiasi dan penghargaan kepada Pemkot Pasuruan.
Sementara itu, Rektor Universitas Jember Drs. Moh. Hasan, M.Sc., Ph.D. dalam sambutannya menyampaikan apresiasi dan penghargaan kepada Pemkot Pasuruan.

 1. Komisi IX RI, setelah mendengar aspirasi masyarakat, tetap konsisten terhadap hasil kesimpulan Rapat Kerja Gabungan Komisi IX dan Komisi XI DPR RI, dengan Menteri Koordinator Bidang PMK, Menteri Kesehatan, Menteri Sosial, Menteri PPN/Bappenas, Ketua DJSN, dan Dirut BPJS Kesehatan pada tanggal 2 September 2019 untuk tidak dinaikkan premi JKN bagi Peserta Bukan Penerima Upah (PBPU) dan Bukan Pekerja (BP) Kelas III.
1. Komisi IX RI, setelah mendengar aspirasi masyarakat, tetap konsisten terhadap hasil kesimpulan Rapat Kerja Gabungan Komisi IX dan Komisi XI DPR RI, dengan Menteri Koordinator Bidang PMK, Menteri Kesehatan, Menteri Sosial, Menteri PPN/Bappenas, Ketua DJSN, dan Dirut BPJS Kesehatan pada tanggal 2 September 2019 untuk tidak dinaikkan premi JKN bagi Peserta Bukan Penerima Upah (PBPU) dan Bukan Pekerja (BP) Kelas III.





{kind=link}